The Patient Body
Accusing the FDA of Playing God
A monthly column by Ann Neumann about issues at the intersection of religion and medicine.
By Ann Neumann
“Compassion impels us to want to help terminally ill people in any way we can, but a less emotional analysis of right-to-try bills, coupled with a knowledge of the science and conduct of clinical trials reveals that these laws, as currently constituted, are almost universally a bad idea.” David Gorski, Science-Based Medicine, July 21, 2014.
Debra Johnson was born with “wads of flesh for thumbs, and her arms were folded up like chicken wings.” With surgery, her index fingers were fashioned into thumbs, her arms were straightened. For 30 years, she thought her deformities were an act of God. “She said she heard the same refrain for decades from doctors and family: ‘That’s how God made her,’” wrote the Philadelphia Inquirer in October, 2013.
As an expectant mother, Johnson feared that her son would be born with the same physical defects, but he wasn’t. When, years later, he went off to medical school, he called his mother one day to tell her that he knew the cause of her birth defect: thalidomide. “I came home that night, and I started looking it up, and the more I read, the more I just cried,” she told the Inquirer’s Reuben Kramer. Johnson joined up with others who were born with birth defects in the same era to sue GlaxoSmithKline (formerly Glaxo, Kline, French) and Sanofi-Aventis (formerly Richardson-Merrill) for distributing thalidomide in the early 1960s, despite knowledge that the drug caused birth defects. In April of this year, a Pennsylvania federal judge dismissed the cases stating that they were subject to a one-year statute of limitations.
Thalidomide was developed in Germany in the sleeping pill-heavy 1950s and entered the market in 1957 as the “only non-barbiturate sedative known at the time,” and therefor safe for pregnant women. By 1960 it was distributed in 46 countries with sales numbers that rivaled those of aspirin, wrote Bara Fintel, Athena T. Samaras and Edson Carias in Helix, a publication of Northwestern University, in 2009. An Australian doctor, William McBride, found that thalidomide also prevented morning sickness in pregnant women, an “off-label” use of the drug, and set what the Helix authors call a “worldwide trend” of use.
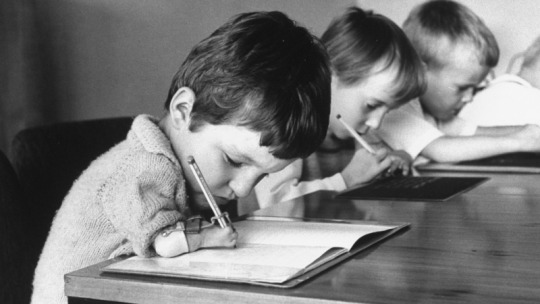
Kindergarteners born with phocomelia as a side effect of the drug thalidomide. (Photo by Leonard McCombe//Time Life Pictures/Getty Images)
There was one person in the US, however, who was not convinced that thalidomide was safe, Dr. Frances Kelsey. In her first month at the Food and Drug Administration in 1960, she was tasked with reviewing thalidomide for approval and sale. Despite broad, accepted use in Europe and elsewhere, she was concerned with reported side effects and withheld approval from the US manufacturer, Merrell. “She refused to be hurried,” wrote the New York Times in an obituary for Kelsey, who died at the age of 101 in August this year:
Merrell stood to make millions and was anxious to get moving. It had tons of Kevadon [thalidomide’s market name] in warehouses, ready for marketing, and 1,000 American doctors had already been given samples for “investigational” research. The company supplied more data, but also mounted a campaign to pressure Dr. Kelsey. Letters, calls and visits from Merrell executives ensued. She was called a fussy, stubborn, unreasonable bureaucrat.
Still, drug manufacturers distributed millions of tablets in the US because, as the Philadelphia Inquirer notes, “clinical trials required little FDA supervision at the time.” Soon McBride, the Australian doctor responsible for widespread use of the drug for morning sickness, began to link thalidomide to a high number of children born with defects. By 1962, the drug was banned in Germany and elsewhere, but not before more than 10,000 babies were born with deformities worldwide.
Merrell withdrew its application from the FDA when the reports of birth defects shook Europe. The FDA’s Frances Kelsey was hailed for her prevention of a similar crisis in the US and was tasked with establishing new protocol for drug testing and approval. Write the authors at Helix:
The tragedy surrounding thalidomide and Kelsey’s wise refusal to approve the drug helped motivate profound changes in the FDA. By passing the Kefauver-Harris Drug Amendments Act in 1962, legislators tightened restrictions surrounding the surveillance and approval process for drugs to be sold in the U.S., requiring that manufacturers prove they are both safe and effective before they are marketed. Now, drug approval can take between eight and twelve years, involving animal testing and tightly regulated human clinical trials.
Despite the effectiveness of these longstanding procedures, many in the US—often those ideologically opposed to government regulation, wedded to federalist interpretations of the Constitution, and allied with right-wing groups and think tanks—continue to criticize both the Kefauver-Harris Drug Amendments Act and the FDA’s role in drug approval. A wave of new legislation, called Right to Try laws, which claim to allow terminal patients access to experimental drugs as soon as Phase I trials are completed, have been passed in 24 states in less than two years. Their popularity is largely based on legislators’ and the public’s misunderstanding of the FDA’s process and on the often misleading but heart wrenching tales told by activists and proponents of the bill.
***
To read Right to Try: How the Federal Government Prevents Americans from Getting the Lifesaving Treatments They Need, a new book by Darcy Olsen, president of the libertarian Goldwater Institute, is to encounter real-life fairy tales about everyday Americans who miraculously overcome impossible circumstances to live happy, healthy lives. The people Olsen writes about are torn asunder by delayed or erroneous diagnoses, impossible long-distance travel for treatment, deadly mysterious disease, and epic, repetitious battles waged with pluck, unfathomable determination, hope beyond hope, and blessed new “cutting edge” drugs. The heroes in these dramas are normal and loving families, desperate mothers who refuse to take no for an answer, and altruistic doctors who defy all limits to lovingly care for their dying patients.
The relentless, detestable villain in these tales is not a host of deadly diseases, nor the travails that these diseases bring to bear on the finances, health or spirit of the families afflicted. It’s not the disparity-defining cost of treatment, so far out of reach for so many. It’s not even the inevitable precariousness of human existence, wracked with disease and predestined for death. The villain in every one of Olsen’s stories is a faceless, heartless, bureaucratic government agency, hell bent on ignoring the afflicted, thwarting their obvious last chances at happiness and health, an organization warped to a mission of denying life to the free and defenseless children of our proud, exceptional nation. This cold, death-fostering villain is identified by a simple three-letter acronym: FDA.
Right to Try is an ode to free market ideals, unfettered individual rights, and a blatant pastiche of American religious concepts that characterize the current conservative-minded political movers in the country. The people Olsen writes about are convinced that any new drug is a promise, a miracle, a healthy future for their child. They thrive on hope and the privilege that, as Americans, anything, even a terminal disease, can be cured by corporate innovation unfettered by government regulation.
Jenn McNary, the subject of chapter one—the subtitle of which is, “How the FDA Let a Mother Save One Son…and Left Her Other Son Die”—is dumbstruck when her son is diagnosed with Duchenne Muscular Dystrophy and the doctor tells her there are no treatment options. Olsen writes, “Jenn was incredulous. There had to be something she could do. This was America, after all. Certainly in this day and age, we have treatments for everything.”
When Christine McSherry’s son Jett is also diagnosed with Duchenne, she tells Olsen, “I was a nurse for a long time. I was very accustomed to finding the solution and giving it to the patient and was shocked to find out that there was no solution whatsoever.”
The book is full of this sort of incredulity, the privilege of believing that Americans are immune to the tragedy of death. Perfect lives and traditional families are interrupted not by the common occurrence of deadly disease but the ineptitude of an uncaring government ready to let them die. Medical cures aren’t rare and unpredictable, they’re blessings bestowed by infallible corporate science. Life is a right. Death, it seems in this cosmology, is not in the Constitution.
“The FDA held the power of life and death,” writes Olsen.
It is this polish of unmitigated, unrealistic hope that characterizes the book. Right to Try reads like a barely-updated, “awe shucks”-inducing 1950s family TV show. Children aren’t born, they “come along.” “Hope appear[s] on the horizon.” Good mothers know what’s best for their children and if they fight hard enough they can keep them from dying. Kids go to Camp Promise and become advocates for legislation to “help others.” Boys like sports, love their siblings and if they fight hard enough, they live. Every new drug is an “historic breakthrough.” “The Lord always provides a way.”
***
“There are times when supporting science-based health policy and opposing health policies that sound compassionate but are not are easily portrayed as though I’m opposing mom, apple pie, and the American flag,” David Gorsky writes at Science-Based Medicine. “Mom, apple pie, and the American flag,” are signifiers of a particular version of American culture, call it the American Dream, that reveres liberty, independence and freedom…for those who can afford it. This version of the American Dream, espoused by Olsen, the Goldwater Institute, and Right to Try laws, hold free-market corporations and meritocracy as a kind of faith. They posit that belief in a go-it-alone approach to survival trumps the safety and well-being of others, those who believe differently or don’t have the same resources.
The visage of bland, sentimental and moral rightness that the book projects—and the promotion surrounding the laws themselves—is of another era; clear, absolute and in keeping with that of other “traditional values” ideals perpetuated so often by today’s social conservatives. Of course, this is by careful, politically-savvy design. Only by blocking any question of the objectives and outcomes of such legislation can proponents use morality to paper over nuance and flaws.
And regarding Right to Try laws, the flaws are many. Not only do the laws not guarantee access to drugs, but they potentially pose a serious danger to both individual patients and a drug approval process designed to protect the health and safety of all citizens. Based on model legislation written by the Goldwater Institute, the laws don’t compel any pharmaceutical company to comply with patient requests. For this reason, bioethicist Arthur Caplan has called them “Right to Beg” laws. Nor do they hold doctors accountable for their recommendations or insurance companies liable for coverage of costs (in fact, in a court of law they probably release doctors and insurers from any future responsibility).
The laws and their surrounding rhetoric misrepresent every experimental drug as “life-saving,” when, for instance, only 5 percent of cancer drugs in Phase I ever make it to approval. “Just because a drug has passed phase I clinical trials does not—I repeat, does not—mean that the drug has been ‘deemed safe by the FDA,’ as the laws claim, writes David Gorski at Science-Based Medicine. Patients in hospice or hoping to enroll will likely be prevented from doing so because of the program’s prohibition of curative treatments.
The larger hazard of Right to Try laws is how they threaten a drug’s approval process with the FDA. Should patients receive experimental drugs and experience adverse effects or die—and this is theoretical; there’s no proof that anyone has yet to successfully receive a drug through Right to Try in the nineteen months there have been such laws—bioethicists, doctors, and pharmaceutical companies fear the repercussions that outcome could have on the drug’s testing and approval. In short, one patient’s campaign to receive a drug could ultimately prevent it from reaching thousands of others whose lives it could save in the future.

President John F. Kennedy gave Dr. Frances Oldham Kelsey the nation’s highest federal civilian service award in 1962, saying she had “prevented a major tragedy of birth deformities.” CreditThe White House
And yet, legislators across the political spectrum love these laws. Every governor, representative or legislator can stand by them, claiming in their support to have helped save the lives of their constituents. Right to Try laws expose the gullibility of legislators, their lack of research or critical thinking, and their faith in moral absolutes. Suckered into feel-good laws with no benefit—or the potential to tragically harm drug safety for all of us—lawmakers have been hoodwinked by Olsen and her proponents into messing with public safety.
Only government has the resources and power to protect public health: that’s the FDA’s charge. Weakening or side-stepping the agency, rather than working with it to better serve the needs of both individual patients (via the agency’s existing Compassionate Use program*) and public safety (through extensive testing measure that began with Dr. Frances Kelsey in the 1960s) can disasters like the birth defects caused by thalidomide be prevented.
***
This, the final installment of the “Patient Body” for 2015, feels like a culmination of several themes I’ve explored over the course of the year. In a review of Anthony Petro’s book, After the Wrath of God, in May, I wrote that, “Moralizing of a particular religious stripe seems indelibly attached to some of the most dire public health issues of our time.” But particular ideas of moral behavior have also been used to shape our public policy, as I wrote about the purity movement in July:
Public health regulations are often a telling barometer of our country’s moral compass, from vaccination laws to the legal drinking age. And no public health category is more fraught with moral minefields than sexual health. Right now, our moral compass is set on shaming and inhibiting the lives of young people, particularly women, by setting up and devoting wads of money to an ideal that will never be achieved.
And in October I wrote about new, anti-abortion laws that seek to prevent the abortion of fetuses diagnosed with Down syndrome. On the surface these laws have been described as necessary to provide more information, but their proponents are more concerned about further limiting access to abortion. “To bioethicists, doctors and reproductive rights activists, however, it’s a new way to inject ideological laws into the patient-doctor relationship. Under the guise of disability rights, these laws target women with shame, distrust and intrusive restrictions,” I wrote.
Right to Try laws show us that ideological attempts to shape public policy are not reserved for sexual and reproductive health. In keeping with the Goldwater Institute’s libertarian, anti-government mission, these laws use the rhetoric of personal rights and independence to subvert government regulation, to bring manufacturers and consumers into closer contact. They pit individuals with certain kinds of access and privilege against the health of the rest of the population—with a moralizing “boot straps” logic that is indigenous to our era. But it’s a faulty logic, too reliant on false hope, too imbedded in nostalgic ideals of self-reliance and a political system more concerned with winning than protecting public health.
In October, California’s governor Jerry Brown became the first to veto a Right to Try law, only a week after he signed Death with Dignity into law. Conservative columnist Wesley J. Smith wrote a short, exasperated post for the National Review at the time, smattered with incredulity and “good griefs.” “A ‘right to die,’ but no ‘right to try and live,’” he simplistically concluded. It’s an embarrassing post. One that shows all the piety and emotions of a movement unwilling—or politically unable—to acknowledge that its black-and-white interpretations of beneficial social governance are sentimental throw-backs, out of step with the serious and nuanced problem-solving government is intended to address.
As the election year rolls toward us, we’ll hear even more flattening of complex health issues into tidy polit-speak about the health of our nation. And as Trump moves the GOP further into non-explicit evangelical territory, the moral objectives professed for public health will only become more coded, more covert, more difficult to detect. Tracing these through lines–and identifying their purposes and outcomes—is not just good politics; it is necessary for the health and safety of all of us.
*The FDA has long had a program that allows patients to access experimental drugs before approval but Right to Try advocates have either ignored it or attacked it’s requesting process as too cumbersome, despite the FDA’s recent revision of the process.
***
Past “The Patient Body” columns can be found here.
***
Ann Neumann is a contributing editor at The Revealer and Guernica magazine and a visiting scholar at The Center for Religion and Media, NYU. Neumann‘s book, The Good Death, will be published by Beacon Press in February 2016.